On 21 July 2002, Ms Masson suffered an extreme asthma attack. An ambulance was called at 22.52 and the first paramedics were on scene at 22.58. On arrival, the paramedics noted bystanders were performing CPR. On examination, Ms Masson was found to be cyanotic, with a respiratory rate of 2 breaths per minute. She was tachycardic (her pulse was 150 beats per minute) and hypertensive (blood pressure 155/100).
The treating intensive care paramedic administered two milligrams of intravenous salbutamol between 22.59 to 23.20. This was twice the dose set out in the Queensland Ambulance Clinical Practice Manual but nothing turned on that. The salbutamol appeared to have a positive effect. She was loaded into the ambulance at 23.14 at which time ‘she had a regular pulse rate of 94, improved but still high blood pressure of 140/100, a respiratory rate of 14 … and her colour was normal rather than cyanosed. Her GCS score remained at six.’ En-route to hospital Ms Masson’s condition deteriorated. ‘By 23.19 her heart rate had dropped markedly to 40 beats per minute, her respiratory rate had reduced to 12 retractive breaths per minute and blood pressure was absent. Cardiac arrest was imminent’. The paramedic administered 100 micrograms of adrenaline and intubated the patient. He also arranged for his partner to stop the ambulance and he ‘conducted an emergency left side thoracostomy’ to relieve a tension pneumothorax. He did not attempt to relieve the right sided tension pneumothorax on the basis that he was now able to get air into her left lung and they were very close to the hospital. Two further 100 microgram doses of adrenaline were also given, so that a total of 300 micrograms of adrenaline was administered before arrival at hospital.
Despite the efforts of the paramedics and hospital staff, ‘Ms Masson lingered, catastrophically brain damaged in around the clock care, for many years before her death in 2016.’ A personal injuries action against the State of Queensland, alleging negligence by Queensland Ambulance Service (QAS) paramedics was commenced sometime before her death. The matter did not come on for hearing until February 2018, some 16 years after the injury. On 23 July 2018, Justice Henry (‘Henry J’) of the Queensland Supreme Court handed down his decision – Masson v State of Queensland [2018] QSC 162 – finding that there had been no negligence by the paramedics involved in Ms Masson’s care.
The Evidence
The court heard from 3 experts in emergency medicine and 1 senior paramedic called for the plaintiff and the same number of experts for the defendant – 6 doctors and 2 expert paramedics in total, as well as evidence from the treating paramedics and people who had assisted Ms Masson at the time of her collapse.
The issues
It is well known that in a case alleging negligence the plaintiff has to show that the defendant owed them a duty of care, failed to provide ‘reasonable care’ and that failure caused their loss or damage.
In this case the issue of duty of care was admitted. The State of Queensland admitted that it, through QAS and the QAS paramedics owed Ms Masson a duty to provide reasonable care to her. The State also admitted that it was vicariously liable for any negligence by its employed paramedics. The issue of damage was not in dispute that is there was no doubt that Ms Masson, if she could prove negligence had suffered catastrophic damage. The value of the damages, if liability was established, was agreed at $3,000,000.
The issues where
- Had the QAS either in the way it wrote its Queensland Ambulance Clinical Practice Manual or trained its paramedics, or the paramedics in the way they diagnosed Ms Masson, understood the manual or applied the treatment guidelines failed to provide ‘reasonable care’? and
- If ‘yes’ did that cause Ms Masson’s catastrophic brain injury or, to put that another way, if the paramedics had given different treatment at the scene would Ms Masson have recovered?
The essence of the allegation was that the paramedics should have administered adrenaline, not salbutamol, when they first arrived and this would have been effective to reverse Ms Masson’s condition, allowed her to breath and would have meant she did not suffer permanent brain damage.
Standard of care
The standard to be expected from an ambulance service and its paramedics is ‘that of the ordinary skilled person exercising and professing to have that special skill’ ([29]). The standard is not determined by simply asking what does everyone else do or, in this case, did the paramedics follow the Clinical Practice Manual. The Manual itself may well suggest sub-standard care.
Adrenaline versus salbutamol
The expert evidence was that adrenanline was required where a patient was in cardiac arrest or was suffering an anaphylactic reaction. Further salbutamol was unlikely to be effective where the patient was bradycardic (ie a slow heart rate), with poor perfusion and poor cardiac output. It was a line ball call. The judge identified the competing issues at [90]-[91]:
At the time of initial treatment Ms Masson was not known to be in cardiac arrest or suffering an anaphylactic reaction, so it was not inevitable that adrenaline should have been administered. Nor was she suffering from conditions known to mitigate against the utility of salbutamol, such bradycardia, decreased perfusion and decreased cardiac output.
Ms Masson was however in extremis, which meant that adrenaline would ordinarily have been the preferred drug to administer, subject to her discrete conditions. Of those conditions her cyanosis and likely acidosis were conditions reinforcing the extremely dire state she was in and tending to confirm the appropriateness of administering adrenaline. On the other hand, her high heart rate and blood pressure were conditions founding a legitimate concern that the administration of adrenaline might worsen her state by plunging her into a dangerous arrhythmia or causing her heart to stop – that is, that it would heighten the risk of death.
The standard of care does not require a guarantee of safety or good outcome, it requires a ‘reasonable response’. His Honour said (at [93]):
I conclude that there would have existed a responsible body of opinion in the medical profession in support of the view that Ms Masson’s high heart rate and high blood pressure, in the context of her overall condition, provided a medically sound basis to prefer the administration of salbutamol to the administration of adrenaline at the time of initial treatment.
The use of adrenaline rather than salbutamol was not clearly called for by the scientific knowledge and state of practice at that time.
The Clinical Practice Guidelines
It was alleged that the paramedics had been negligent for not following the QAS clinical practice guideline. A flow chart was included in the guidelines, reproduced in the judgement and copied, below.
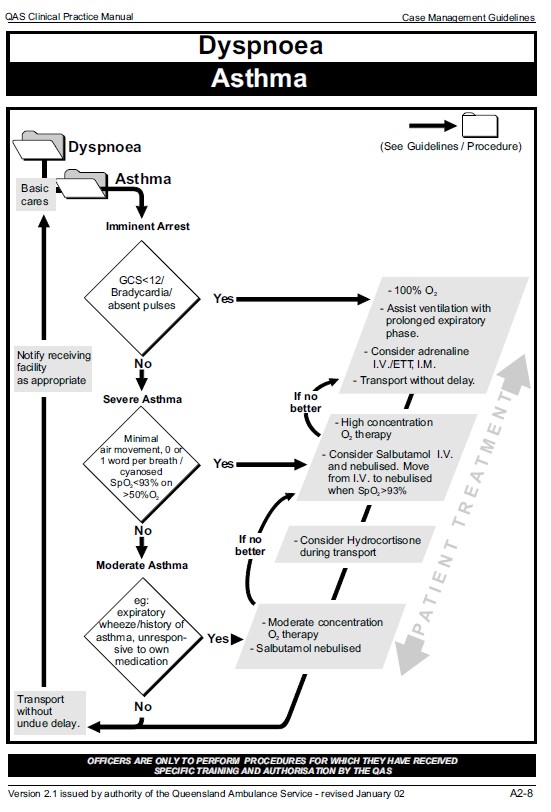
The plaintiff argued that even though Ms Masson may not have been in cardiac arrest she was in respiratory arrest and therefore she was ‘in arrest’, and if the words ‘Imminent Arrest’ meant only cardiac arrest that was indeed ‘imminent’. Second her Glasgow coma Scale was less than 12 and therefore the treatment should have proceeded along the ‘yes’ arrow and that called for the administration of adrenaline.
The defendant, QAS, on the other hand, argued that she was no bradycardic or with absent pulse so the criteria for ‘yes’ were not met; but even if they were the guideline called on the paramedic to ‘consider’ adrenaline, it did not mandate its use.
The judge said they were both right, and they were both wrong. First the list of indicia (GCS<12, Bradycardia/absent pulses) were meant to be read as ‘or’ (not ‘and’) so the presence of any one may indicate that the appropriate answer to the first decision point was ‘yes’. This was also consistent with the actions of the paramedics who did give 100% O2 and did use positive pressure ventilation to assist the patient’s ventilation. In that sense the plaintiff was correct, Ms Masson was in respiratory arrest (even with a respiratory rate of 2 breaths per minute) and had a GCS<12, she was ‘in extremis’ so at the first decision point the answer was ‘yes’.
But even though the answer at that first decision point was ‘yes’, that did not mandate the use of adrenaline, it required the paramedics to consider its use. The judge noted that the Case Management Guidelines were indeed guidelines, he said (at [96]):
It is noteworthy that on the manual’s own terms its case management guidelines are not proscriptive and rather are provided to guide and assist patient diagnosis, management and care.
In a statement the treating paramedic referred to ambulance protocols, Henry J said this evidence:
… curiously introduces the term “protocol”, which is not a term used in the manual. I doubt it is term favoured by [the paramedic], whose evidence showed he understood a protocol requires the taking of a fixed course whereas a guideline permits a greater flexibility of response allowing for the application of clinical judgment.
It was also said, given Ms Masson’s tachycardia and hypertension, that the Case Management Guidelines and/or the Clinical Practice Manual chapter on pharmacology did not permit the administration of adrenaline. Henry J referred (at [149]) to ‘the curious and erroneous references in … evidence to the asthma guideline prohibiting or not permitting the administration of adrenaline’. The indications for adrenaline (eg – Bradycardia) did not rule out its use in other circumstances.
The purpose of the Clinical Practice Manual was to ‘… provide Queensland Ambulance Officers with a comprehensive guide to prehospital clinical practice’. The Case Management Guidelines ‘… provides diagnostic patterns of each listed condition to assist in arriving at an ambulance provisional diagnosis, and guiding principles to assist in patient management’. They were not intended to be prescriptive but to leave room for clinical judgement.
No negligence
In this case the treating paramedic was faced with a dilemma that the various medical experts noted. Ms Masson was critically ill, there was a choice between salbutamol and adrenaline. Some symptoms called for adrenaline, other signs and symptoms suggested it was not safe to use. Answering ‘yes’ to the question was arrest imminent required the treating paramedics to ‘consider adrenaline’ and the evidence was that they did consider it, and ruled it out. At [151] Henry J said:
The asthma guideline did not require adrenaline to be administered. It prompted consideration of the administration of adrenaline. The administration of adrenaline was considered but rejected by reason of the concerning presence of tachycardia and hypertension. The presence of those conditions would have been regarded by a responsible body of opinion in the medical profession as supporting the view that Ms Masson’s high heart rate and high blood pressure, in the context of her overall condition, provided a medically sound basis to prefer the administration of salbutamol to the administration of adrenaline at the time of initial treatment. Opting to administer salbutamol in preference to adrenaline in those circumstances was a reasonable response to the known risks.
And at [155]:
The treatment which was administered did not fall below the standard of care to be observed by ambulance officers and was not contrary to the QAS asthma guideline. No breach of the duty of care has been established and the claim must fail.
Causation
Finding that there had been no breach of the standard of care is the end of the case, but His Honour went on to consider whether, if the decision not to administer adrenaline had been negligent, there was evidence to support a conclusion that this was a cause of Ms Masson’s brain injury. He did this to deal with all the arguments and if there is an appeal, and the Court of Appeal holds that his reasoning on breach of duty was wrong, then this issue has been determined and a further trial isn’t required.
On causation Henry J noted that Ms Masson had a history of severe asthma attacks and these had been resolved in hospital or by paramedics with the use of adrenaline. The treating paramedics in this case did not know that history but it was evidence to suggest that if adrenaline had been used, it may have been effective. His conclusion is at [182]:
While the issue is finely balanced, I conclude that if, contrary to my findings, there was a breach by reason of a failure to administer adrenaline during the initial treatment, that breach was likely a material contributing cause of Ms Masson’s injury. Put differently and aided by information the ambulance officers did not have, I conclude on the balance of probabilities that it was not too late at the time of initial treatment for Ms Masson’s injury to be avoided by administering adrenaline.
That is if the decision not to use adrenaline had been negligent, he would have found that it did cause or significantly contribute (which is all that is required) to Ms Masson’s ultimate injuries.
Is it over?
Not quite. The usual rule is that the loser has to pay the winner’s legal costs. At [191] Henry J said ‘While costs would ordinarily follow the event, I will out of caution give the parties an opportunity to be heard’. The matter returns to court on 8 August 2018 for final orders as to costs.
That will be the end of the matter unless the plaintiff choses to appeal. They cannot appeal just because they do not like the result. They can only appeal if they can argue that the judge made a mistake in his interpretation of the evidence, analysis of or application of the law. Whether they will seek to appeal, I cannot say.
Discussion
This was the decision of a trial court so it does not set a precedent (see Accessing a judge or magistrate’s reasons for decision (November 18, 2016)). Even so it says somethings that, apart from the actual result, will be of interest to paramedics and readers of this blog.
First, there is much debate about the meaning and extent of vicarious liability. Coming through is the hidden subtext that employers will through employees ‘under a bus’ at the first opportunity. I even read on one forum a claim that if a nurse is found to wear the wrong shoes to work, the employer will be able to escape liability. That is, of course, nonsense. Whilst in this case the defence was that the paramedics had indeed followed the guidelines and protocols it is worth noting that there was never any doubt that win or lose, it was the state of Queensland, not the paramedic who would be liable.
Second the case reinforced the professionalism and the authority of paramedics to make clinical judgements. In Queensland at least, the Clinical Practice Manual and Case Management Guidelines are indeed guidelines, intended to facilitate good clinical decision making, not to prescribe what is to happen in each case. As the guidelines said in 2002 (at [98] with emphasis added by Henry J):
Officers must consider the best possible care for the patient. The QAS Clinical Practice Manual is designed to assist clinical judgment, using the problem solving approach, to achieve best practice. It is acknowledged that every situation is different. Deviations from the guidelines will occur but must be documented and audited, and officers must be able to justify that their treatment was in the patient’s best interest.
Paramedics in 2002 were not automatons but trusted medical professionals and that is even more the case in 2018 as evidence by the move to bring paramedicine under the national registration scheme for health professionals.
Third and finally, the case demonstrates the sheer inefficiency of a legal system that allows a case like this to take 16 years for finalisation. For everyone involved having these proceedings take so long must simply compound the tragedy that ended in Ms Masson’s death. The treating paramedic was writing statements 7 years after the event and giving evidence, and being asked to recall his clinical decision making process 16 years after the event. It is not surprising as Henry J noted (at [146]):
The tone and manner in which … answers were given made it obvious that [the treating paramedic] had difficulty, doubtless because of the very long lapse of time (if not perhaps the contaminating contributions of others in legal forums), in distinguishing between hindsight assumption and actual recollection.
That was not said as a criticism, just a reflection on the reality of the situation.
If Ms Masson’s estate had won this case there would have been a verdict for $3 million but that would not have been a windfall for the estate. From 2002 to 2016 Ms Masson received 24 hour care. That was paid by someone, probably Medicare, Commonwealth social security, private funds or other forms of social welfare. Expenses that have been met by Medicare or Social Security have to be repaid. It is often the case that even with large dollar amounts for compensation, all that a claim for damages does is transfer money from the insurer to various government agencies that have been providing support. Queensland’s insurer may have avoided paying $3 million in damages but with the time taken, the legal fees, the cost of the 8 expert witness, the costs of providing the court, the judge and the court staff, one can’t help but think this case already cost $3 million. Diverting all that money to meet the needs of those with catastrophic injuries rather than trying to decide who’s to blame may be a more useful way to spend the money.

Hear hear! Well said Michael. We have no-fault compensation schemes for motor vehicle and workplace injuries so why not for medical matters. That would mean that funds can go where they are most needed ie the patient. Any issue of professional conduct can be dealt with by professional regulator.
Hi Ruth, motor vehicle accident compensation is not universally no fault. Here in the ACT it’s very much fault based as it is in NSW. The country is introducing no fault catastrophic injury compensation based on the NDIS for motor accidents but it won’t cover everyone and is not yet fully in place.
It’s terrifying to watch people deteriorate and die from severe asthma attacks. Kudos to the Ambo team who evidently did their best to try help this poor lady. It’s always easy to critique in hindsight. There are no absolutes in clinical medicine; we can write as many guidelines as we like, but at the end of the day it all comes down to making that best clinical judgement in that moment based on whatever limited information we have to work with.